Immunology is hard, people. I was a fantastic student right up until Immuno-Genetics, where my C- from Naomi Rosenberg was a passing gift. True story: I could not answer most of the questions, so turned the test over and word-vomited all of my memorized notes alongside an apology for being an idiot. Those of us who ultimately earned our PhD in Immunology specialized in small pockets of a gigantic field. For four years, I studied the effect of a single protein on the ability of white blood cells to travel through the body. One protein. But for four years, I also attended weekly lectures, dissertation presentations of fellow graduate students, conferences, journal clubs, and even shared an apartment with another immunologist. Nicole and I didn’t pour wine, we aliquotted. We also digested a lot of theories, factoids, terminology, and problem-solving mindsets from the geniuses that taught us. I defended my thesis over 20 years ago, and somatic hypermutation and cluster determinants have not been close to the tip of my tongue since then. But as SARS-CoV-2 began its course across the planet, it all came rushing back with one great truth: Immunology is hard, people.
I’ve never been hopeful for a COVID-19 vaccine. And after visiting the Facebook page of my own community after our state mandated flu vaccines for kids in childcare and schools… well, even if Fauci backed a vaccine for COVID-19 today, many would opt out, anyway. Why? Thoughtful people worry that a quickly produced vaccine might not be entirely effective or safe, and let’s be honest; most people prefer to avoid any shots at all. But instead of saying those things, it’s juicier click-bait to blame an unpopular President for seeding mistrust in our scientists. In any case, the upshot about a pandemic-squashing vaccine is first that it is unlikely to be developed soon, and second that it will be harder to attain herd immunity with it than anyone assumes.
An oft-repeated argument against acquiring a flu shot right now is, “Why would I overtax my immune system during a pandemic?” This causes immunologists to face-palm, but they’ll seldom chime in to correct this vein of thinking. Again, Immunology is hard, people. Also, anti-vaxxers of all varieties are especially combative in on-line settings and paradoxically immune to PubMed searchable corrections. But as an immunologist, it sounds like this to me: “Why would I get my oil changed when I need new brake pads?” Your immune system is diverse and complicated with myriad weapons; it can react and remember. It uses too many different cell types and mechanisms to recount here. Quite simply, though, a recently published systematic review showed that COVID-19 is associated with certain co-infections–Influenza types in particular, for which we have vaccines– that increase mortality in those patients. (Bacterial infections are also common in our sickest COVID-19 patients, but we have antibiotics to treat those.) We also want to keep preventable diseases to a minimum during a pandemic. My hunch is that a flu shot/mask-wearing combo will stifle a significant number of flu cases and hospitalizations. Yay!
But how do we get back to Life as We Knew It?
We’re back in Zoom School here at the Lee house, and it feels like March all over again. My boys log in with bedhead, want lots of different snacks and meals at different times, and are always around except when the puppy needs walking. Their school put together an incredibly thoughtful plan that puts boys on campus with their cohort every other week. With masks and Purell stations and extreme vigilance (I’m looking at you, sportos with your outta state tournaments) we might get the whole school back in person before lacrosse season. Unfortunately, the only tools we have right now are self-evaluation (which requires diligence and honesty), hand washing (ditto), masks, and social distancing (which we’re fudging a bit inside the schools).
What if we could just test ourselves every day before leaving the house?
The greatest minds in epidemiology and virology tell us the only way we’re going to stop SARS-CoV-2 from reappearing and spreading in hotspots for years to come is to battle the RT into submission by keeping people who are actively shedding virus—whether they display symptoms or not—from leaving their homes. Dr. Michael Mina has been a vocal expert and advocate for technology that already exists: a home administered saliva test that takes 15 minutes. No, it’s not as sensitive as the PCR assay that amplifies the actual viral genes. Instead, it detects a certain threshold of antigens: those sticky proteins on the outside of the virus. Your positive Rapid Antigen Test would mean you are COVID-19 positive and also suggest that you are extremely infectious. Of course, those who test positive with the home test would follow up with a PCR test and a doctor’s visit (more data, yay!), and those who test negative and have no symptoms could go to school, a restaurant, or the movies. There will be some gaps with false negative tests, but with daily testing the chances of missing positive cases are reduced each day (yay, math!). Also, there will be far fewer false positives than the PCR assay, which is likely keeping people quarantined longer than necessary.
Experts predict that we could get our pandemic under control in as little as six weeks with widespread, daily rapid antigen testing. Meanwhile, we could more confidently open schools and gyms, see people outside of our bubbles, and worry less about killing grandma. The only things stopping this is red tape, money (ok, so a heady sum of $), but ultimately… The American Spirit. Explaining the inexpensive ease of daily testing to my own smartypants big sister was met with, “meh… sounds like a lot.” Even when I explained that it could cost $1 and take 15 minutes, she, like so many of us, is just over it. We have a collective pandemic fatigue that is making us skeptical and more and more willing to turn a blind eye to the thousands (millions?) more who will die if we don’t do something.
Enter Dr. Scott Atlas. He’s likely brilliant and certainly has better credentials to speak about the pandemic than the average Twitter ALL CAPS hand-wringer, but he doesn’t have any more expertise in Virology and Immunology than the guy reading your MRI. Nonetheless, he caught the eye of our President who is looking for different solutions, even if they might not be better. If you do a quick search, you’ll find that Dr. Atlas is advocating “herd immunity” to spare the economy and advance his career. That’s the problem with the quick search and also the leading motto of this essay. Immunology is hard, people. I think he’s being largely misquoted, but his stance on masks is just irresponsible. Either way, NYT reporters (none is a scientist) attempted to malign him today by reporting that his theories about T cell mediated immunity are considered bunk by immunologists. They even sourced a TWITTER THREAD that includes peer-reviewed papers of immunologists hopefully speculating about a role for T cell memory. They need more data, but they certainly don’t think it’s bunk. How did they get this wrong? First, they only read the first tweet of the thread. Second, IMMUNOLOGY IS HARD, PEOPLE. Finally, those of us who consider ourselves any sort of scientist are horrified about any of this being politicized. And sourcing a Twitter thread as a scholarly reference? And misinterpreting it? Naomi Rosenberg is going to give this less than a C-.
Wash your hands, wear your mask, socially distance as much as possible, and be honest about your comings and goings. But if you want to get back to something akin to Life as We Knew It, text RAPID CONGRESS to 50409 to support the development of inexpensive saliva COVID-19 testing that can be done at home!
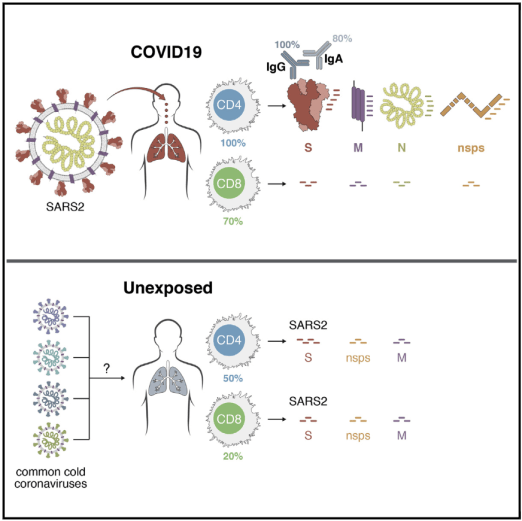
IMMUNOLOGY IS HARD. This group detected SARS-CoV-2-reactive CD4+ T cells in 40%–60% of unexposed individuals, suggesting cross-reactive T cell recognition between circulating “common cold” coronaviruses and SARS-CoV-2. THIS IS GOOD NEWS!